
Prof. asoc. Dr. Stefan Gress
Plastic & Aesthetic Surgeon




Vaginal Tightening
Professor Gress is one of the
top specialists internationally

Welcome

How to find the right doctor?

Whats next?

How is the procedure performed?

The days after surgery

Risks and complications
What would you like to find out more about?
Vaginal narrowing, vaginal tightening
directly proportional to the friction forces during sexual intercourse.
It goes without saying that a small penis in a large vagina creates little pleasure.
This is a phenomenon that affects women immediately after pregnancies ending in vaginal deliveries. Perhaps it was not really that intense before, but now it is even less so: vaginal stimulation during sexual intercourse!
Sexual stimulation is heavily dependent on the intensity of mechanical friction along with a whole host of other factors. If the friction is not strong enough, the stimulation is too weak, especially in order to reach climax. If it is too strong, it can cause pain. It goes without saying that a small penis inside a large vagina is not very pleasurable.
Many couples suffer as a result of this fact. It is not uncommon for couples to split up because a significant component of the life they share together as husband and wife has dwindled.
A harmonious partnership cannot, of course, be reduced to sexual satisfaction and pleasure alone. Nevertheless, the desire for sexual fulfillment is one of the greatest and most basic human needs. A harmonious and thus sensual partnership requires the ability to both enjoy pleasure as well as give it.
As women age, anatomical changes can be considerable, especially after childbirth. Filling out a very stretched vagina,hen, is a difficult feat for a man with an average-sized penis.
Adapting a penis to these changes through surgical means is not possible. Although it can be lengthened to some extent, it is not possible to effectively increase its girth.
However, narrowing the vagina and resetting it along with all the structures that have been stretched and lost their tension over time is certainly a possibility. The end result aims to replicate the anatomy of a youthful woman who has not yet had a vaginal delivery, creating the conditions for optimal sexual stimulation.
The aim is to increase frictional pressure during sexual intercourse as much as possible.
It is merely an anatomical change that returns your body to the condition it was in before giving birth – or even better. However, if you are no longer sexually attracted to your partner, there is not a great deal we can do!
After a physical examination and some questions regarding your medical history, which focuses primarily on your gynecological situation (especially the number and type of births), we will suggest and discuss with you the therapy that we feel would be most promising for you.
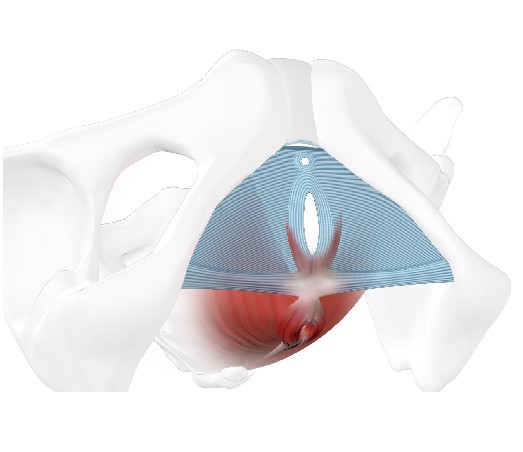
Pelvic floor
A large number of organs are located in the pelvis, which is shaped like a ring: the rectum, the bladder, the vagina, the ovaries, etc.
In order to stop these organs from slipping down, a kind of hammock is stretched out within the pelvis: the pelvic floor. It essentially comprises muscles (Levator ani muscle) and fascia (connective tissue plates, similar to the structure and density of a muscle tendon).
At its core, there are openings for the passage of the intestines, the vagina, and the urinary tract.
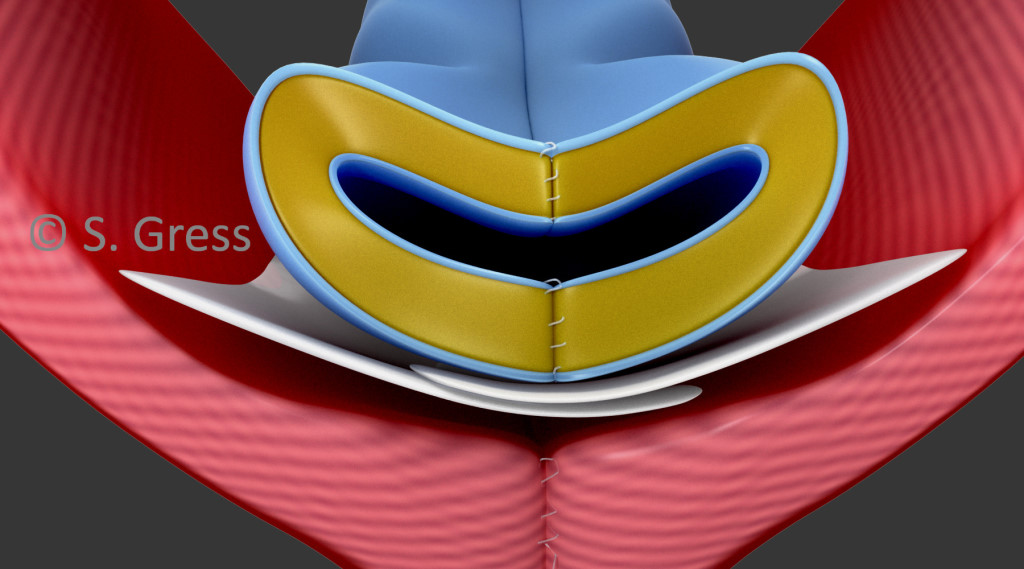
Pelvic floor:
Red section: Levator ani muscle with passage of the intestines (anus)
Blue section: Fascial plate (urogenital diaphragm) with passage of the vagina and urethra
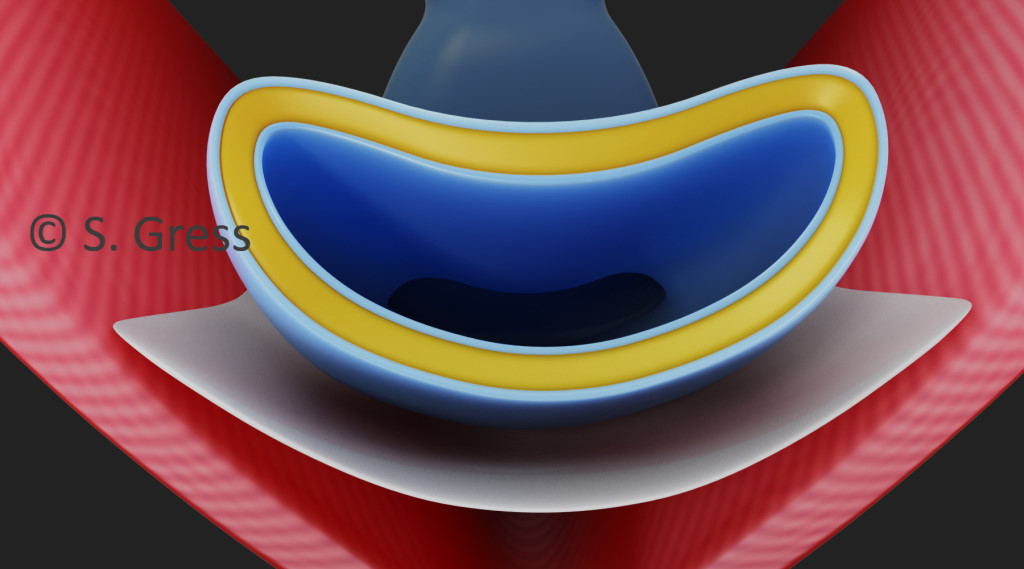
How?
Principle of the procedure (vaginal surgery)
Anatomically speaking, the vagina is like a tube and is the counterpart to the penis. If the vaginal tract is too wide, it is surgically possible to narrow it. However, narrowing the vagina by removing skin alone would not be sufficient as vaginal skin is very elastic – how it is designed to be for childbirth. As the skin is stretched again, e.g. during sexual intercourse, the result would therefore not be a permanent solution (that is why lasers that purport to tighten the vaginal skin do not really work!).
It is important that the muscles surrounding the vagina (pelvic floor muscles) are also tightened so that external pressure can be applied to the vagina, thus preventing the vaginal skin from stretching excessively again. Additional padding and thickening of the vaginal wall using autologous fatty tissue intensifies this effect.
The procedure involving these three steps provides the optimal anatomical basis for ideal sexual stimulation. It goes as far as is medically possible and is extremely successful and effective. We are proud to be able to say that, up to this point, every patient has been highly satisfied with the results of this operation.
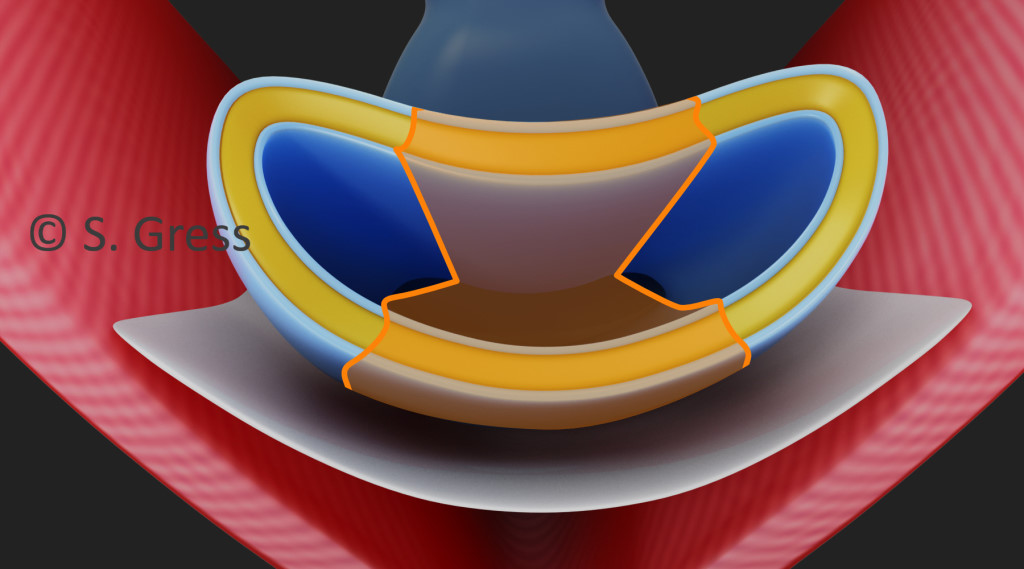
The individual steps of vaginal narrowing (vaginal rejuvenation)
1. Narrowing the vaginal canal Vaginal skin is removed from the posterior wall of the vagina. Tissue can also be taken from the anterior wall if the vagina is very wide and the patient is experiencing urinary incontinence. Tightening the anterior wall of the vagina simultaneously lifts the base of the bladder, treating incontinence problems.
2. Tightening the pelvic floor muscles and fascia This provides the vagina with external pressure, support, and firmness. It is straightened up again, just like in your younger years. This is the vital step that ensures the long-term success of the treatment and counteracts renewed overstretching of the vaginal skin.
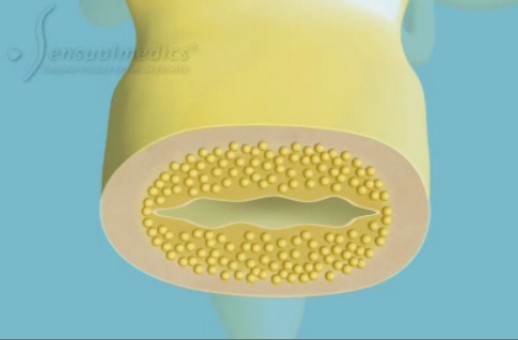
3. Padding and thickening the vaginal wall with autologous fatty tissue Fatty tissue is a wonderful filler that can be used to create volume. Injecting the body’s own fatty tissue into the vaginal wall thickens and pads it out without the need for additional incisions and scars.
The fatty tissue is removed from the (outer) thighs or the inside of the knees, specially prepared, and injected circularly into the middle section of the vagina (the most sensitive part of the vagina) through thin cannulas under the vaginal skin.
The duration of the procedure is around two-and-a-half hours and is performed on an inpatient basis at the clinic. The inpatient stay is two nights.
Vaginal Tightening:
Vaginal narrowing using autologous fat injections alone
This is a very elegant method of vaginal tightening that requires no incisions and leaves no scars. However, the extent to which the vagina can be narrowed is limited. A narrowing of around 20% can be achieved by injecting autologous fat.
This is the method of choice for women who have not yet given birth and want improved vaginal stimulation!
However, after a vaginal delivery, this therapy is not very effective as the overstretching of the tissue caused by childbirth is not corrected to a satisfactory level and a vaginal narrowing of around 20% does not usually go far enough to achieve a noticeable change.This procedure can be performed under local anesthesia on an outpatient basis. Major aftercare is not necessary. Sexual intercourse is permitted again after two weeks.

Vaginal narrowing including the tightening of the pelvic floor muscles is performed under general anesthesia as part of a two-day inpatient stay. Narrowing is performed under local anesthesia on an outpatient basis by means of autologous fat injection alone.
In any case, you should not take any blood-thinning medications (e.g. aspirin, etc.) 14 days prior to the procedure.
An extensive preliminary examination is necessary in all cases. You will receive all the important information on how to prepare for each procedure.
Vaginal narrowing including tightening of the pelvic floor muscles
- Protection of the pelvic muscles for six weeks (no
- heavy lifting, no straining on the toilet, etc.)
- Removal of the tamponade and bladder catheter the day after the procedure at the clinic
- Discharge from the clinic on the second postoperative day
- No sexual intercourse for six weeks
- Drink plenty of fluids to ensure soft bowel movements
- Check-up after six weeks
Vaginal narrowing using autologous fat injections alone
– Check-up and dressing change the day after the procedure at the practice with removal of the vaginal tamponade
– No sexual intercourse for two weeks
Prof. Gress has published most of his medical publications with Springer Verlag.
His textbook on correcting the outer female genital region entitled „Aesthetic and Functional Labiaplasty“ was published in 2018.
This book describes his techniques for reducing the labia minora, primarily the “composite reduction labiaplasty”, and techniques for correcting the labia majora and the mons pubis. This textbook is now the standard for colleagues in this field throughout the world.
Publications by Prof. Gress:

(click for further information)
Good to know
alle wichtigen Fragen
Insurance
Statutory health insurance providers shall only bear the costs, if at all, in accordance with their rates and after examination by the medical service. We do not work in partnership with any of the statutory insurance companies.
Private insurance companies, on the other hand, are less restrictive and cover part or all of the costs if there is a medical indication. A medical indication exists if there are functional impairments, such as significant impairment of sexual function, urinary incontinence, etc.
It is advisable to inquire in advance with your insurance company whether or to what extent the procedure is covered. We would be happy to provide you with a cost estimate.
Costs and operating time
Vaginal narrowing, tightening the pelvic floor muscles, and lining the vagina with autologous fat:
EUR 8,800 plus anesthesia and clinic costs for inpatient accommodation. The procedure is exempt from VAT as there is a medical indication. There are also costs for anesthesia and inpatient stay for two nights.
Operation duration is around two-and-a-half hours.
Filling with autologous fat:
EUR 2,900. The procedure is exempt from VAT as there is a medical indication.
Operation duration is around one-and-a-half hours.
The fee for the operation must be settled before the day of the surgery. A deposit of EUR 500 is required to secure an appointment for surgery.
Sutures, stitches
The stitches are made of absorbable sutures and do not need to be removed.
Risks
There are no serious risks or complications associated with a vaginal tightening. Severe pain is not to be expected; patients may experience a slight to moderate feeling of pressure on the perineum, but this quickly subsides. You should drink a large glass of water daily, especially before breakfast, to ensure soft bowel movements. Once the bladder catheter is removed the day after the procedure, you should be able to urinate independently again. However, if patients have more severe swelling, this can prove more difficult, meaning the bladder catheter must remain in place for a little longer. But this is very rarely the case.
Is vaginal laser treatment an option?
In short:
Vaginal laser treatment (ThermiVa, FemiLift (Alma), CO2 Laser etc.) is either useless or harmful for vaginal tightening!
The industry soon realized that the desire for a fulfilling and stimulating sex life is a huge market. Not so long ago, various lasers and instruments resembling dildos were developed for insertion into the vagina to achieve a narrowing of the vagina primarily through heat and warmth to simulate the effect of surgical vaginal tightening or narrowing.
As already mentioned, sexual stimulation is mainly about friction. If the friction is not strong enough, there is no stimulation. The main reason for this is a disparity between the size of the vagina (more precisely, its diameter) and the penis girth. If the vagina and pelvic floor muscles have been greatly stretched after childbirth, it becomes difficult or impossible even for a man with a very large penis to fill the vagina and create friction through movement.
Vaginal laser treatment promises a shrinking effect on the vagina using heat. The aim is to contract the collagen fibers of the vaginal skin and thereby narrow the vagina in order to create stimulation again. The fact is, however, that only intense heat has the effect of tightening the skin and shrinking collagen fibers. The heat must be such that it burns or scalds the skin, corresponding to a second-degree burn. However, this would irreversibly damage the skin blood flow and also the sensitive nerves. The skin dies, necrosis develops and there is scarring with loss of sensation instead of soft, sensitive vaginal skin. This type of damage is irreversible. The heat from vaginal lasers offered for this purpose is therefore relatively low, producing only temporary irritation and reddening of the vaginal skin, and is therefore useless. These treatments are very expensive and have to be repeated at intervals, with the intention of eliciting even more money from you…
Vaginal narrowing through lasering the vaginal skin alone?
The industry has long since discovered the market for female genital surgery and developed vaginal lasers that promise to produce a tightening effect simply by applying impulses to the skin of the vagina. Our experiences with this technology have been anything but positive! If the vagina is very overstretched, only very little effect or none at all can be felt. The costs are high.
This method has been discontinued from our range of treatments due to its inefficiency!
Laser or scalpel?
We perform the procedure using a radiofrequency surgical device. Similar to a laser, the tissue is cut using thermal energy; however, the tissue is separated through contact between the wire and the skin, instead of a light beam. The advantage is that any trembling of the hand is not transferred to the incision line, as is the case with a laser.
Childbirth
If you are planning to become pregnant after vaginal tightening, it is advisable not to attempt a vaginal delivery but to undergo a cesarean section, as otherwise the result of the achieved narrowing would be reversed.
A vaginal delivery is no problem after an autologous fat injection alone.
Periods
Having your period on the day of surgery does not constitute a problem. You should, however, remember that you cannot use a tampon for four weeks, only a sanitary pad.
Pain
We will issue you with a prescription for two effective painkillers to treat your pain. These should prove sufficient. Patients usually experience moderate pressure pain in the perineum after vaginal tightening. This is caused by the suture in the pelvic floor muscles. This does, however, only last for a few days.
Swimming
You should avoid chlorine-treated water in public swimming pools for three weeks. You are allowed to swim again in lakes or the sea after one week.
Showering, water, soap
You can take a shower after two days, but may only use clear water for one week. Please only use pH-neutral products. Do not take a bath as this would soften the wound edges!
Sexual intercourse
Sexual intercourse is permitted six weeks after vaginal tightening, but only after the check-up at the practice.
If the vagina has been narrowed using autologous fat injections, you can resume sexual intercourse after two weeks.
Sport
You should not do any strenuous sports or lift heavy loads for six weeks. Protect your pelvic floor muscles!
How many appointments do I need?
For inpatient vaginal tightening procedures (tissue tightening, pelvic floor surgery), you will need three appointments: consultation/preliminary examination, surgery and, a follow-up examination about six weeks after the operation. The consultation and surgical procedure may not take place on the same day. There should be an interval of at least 7-14 days between the consultation and surgery so that you can take your time to think about the operation.
For outpatient vaginal tightening procedures (padding with autologous fat), you will need a total of three appointments:
consultation/preliminary examination, surgery, and a follow-up examination the morning after the operation. The consultation and surgical procedure may not take place on the same day.
Success of treatment
As described above, a study by Master and Johnson revealed that the degree of pleasure gain is directly proportional to the frictional forces being applied during sexual intercourse.
The aim of the procedure is to correct existing vaginal dilatation and to create an anatomical situation that allows vaginal stimulation to be enjoyable again.
Experience has shown that the procedure can significantly improve and increase the stimulation ability of both women and men during sexual intercourse, making sex pleasurable again for both.
Of course, this cannot be guaranteed, just as the success of medical treatment can never be guaranteed. That said, vaginal narrowing with pelvic floor tightening in particular is extremely successful when it comes to the ability for sexual stimulation. We are proud to be able to say that, up to this point, every patient has been highly satisfied with the results of this operation.
However, if you are no longer sexually attracted to your partner, there is not a great deal we can do!
The right treatment
The type of procedure can only be decided after a physical examination, in which the degree of vaginal laxity is determined.
If the aim is to achieve only a discreet narrowing of the vagina, injecting the vaginal wall with autologous fatty tissue can achieve the desired effect. This is usually the method of choice for women who have not yet had a vaginal delivery.
In the case of more extensive dilatation, the vagina may need to be tightened by tightening the pelvic floor muscles. If the patient is also experiencing incontinence problems (involuntary bladder voiding), they will require vaginal pelvic floor tightening including lifting of the base of the bladder.
Hotels
We will be glad to help you find a suitable hotel of any kind. We have a partnership with Hotel Vier Jahreszeiten Kempinski, Munich, which means our patients are offered more favorable rates. They should, however, refer to our practice when booking the hotel or make the booking with our assistance .
Shaving
Please completely shave your genital area before the procedure.
Working
You can return to work the day after the procedure.
Financing
Please understand that we are unable to provide any financing ourselves. However, MEDIPAY has been our reliable partner on this matter for many years now. You can find all the relevant information by clicking on the following link www.medipay.de.
Individual information
You can request further information or arrange an appointment here. This is non-binding information free of charge. We have set up a telephone advice service for you. Call +49 (0) 89 24 22 39 22 for advice on your own surgical needs. This personal advice service is non-binding and free of charge.
Best Results
by specially developed, internationally leading surgical technique “Composite Reduction Labiaplasty”

Greatest Experience
With the most operations in
the female genital
area worldwide
Media Partner
First point of contact for international media for all questions relating to intimate surgery
Prof. Dr. Gress
Experience makes the difference
- More than 6700 procedures in the female genital area
- Over 20 years of experience
- Inventor and developer of the “Composite Reduction Labiaplasty”
- Internationally recognized top specialist
- Author of the international textbook “Aesthetic and Functional Labiaplasty” (Springer Publishers)
- Professor and Lecturer in Plastic Surgery


„Pioneer of female genital surgery“
„The Vagina Picasso“
„The labia pope of Germany“
Memberships
In the most important national and international specialist societies
American Society of Plastic Surgeons
Deutsche Gesellschaft der Plastischen, Rekonstruktiven und Ästhetischen Chirurgen
International Confederation for Plastic, Reconstructive and Aesthetic Surgery
International Society of Aesthetic Plastic Surgery

The Aston Baker
Cutting Edge
Aesthetic Surgery
Symposium
2018, New York
Faculty Member
The greatest honor for
a Plastic Surgeon
Aesthetic and Functional Labiaplasty
The internatioanl Textbook
written by Prof. Gress

Published in January 2018 by Springer Verlag, it has developed into an international bestseller and standard work in plastic surgery
Well known from the Media












